Shanksteps Bere April #9
It rains near by in the early evening and the air cools from 95 to about 86. I sleep well. I am called at 5:30 to see a woman who is 26 years old with RLQ pain since last night. She says the pain is constant and strong. She points to her Right flank. She’s vomited a couple times. Her tests show she has malaria and doesn’t have typhoid. Though I know the type of typhoid test we have here is very inaccurate. She also is not pregnant. She denies any vagnial discharge and hasn’t had any problems with BMs or urination. I ultrasound her and see a normal appearing kidney on that side. I can’t see an appendix. But based on her symptoms I think this likely represents appendicitis. So I ask them to keep her NPO (nothing per Os. Nothing by mouth). Get an extra IV going and we will plan on operating on her this morning.
Later on Im told she is feeling better and doesn’t want surgery. I think good, maybe I was wrong. Then I see a text from Dr. Staci, appy lady, have I seen her. She sends her over to the OR where I’ve been all day. As I examine her she says she feels somewhat better and doesn’t want an operation. I take this as a good sign, and decide Ill examine her again in the morning.
My first surgery this morning was an old guy with prostatic hypertrophy for a prostatectomy. I wish I new how to do a TURP and had the equipment. That would be best, but I do what I know how to do and it does help them. I do tow old guys today in the same manner as Ill describe now. They get a spinal anesthetic. Then fluid is put into and distends their bladder displacing the intestines up and so when I cut down in the lower abdomen, I get to bladder rather than intestines. His abdomen is prepped then I cut through the various layers to the bladder. I sweep the peritoneum (covering of intestines) up and out of the way. Then I open the bladder, sucking all the fluid that we had just put in there. I stick my finger in the bladder and feel a large prostate. Slowly I shell it out. There are two large pieces. My fingers and ligaments ache a bit as they really get taxed when I do this. I close the bladder in two layers and then leave a sterile piece of glove as a drain, and close the rest of the layers.
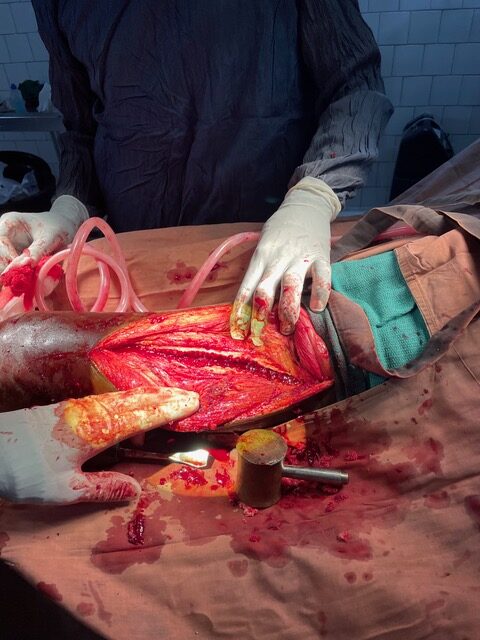
The next is a woman who has cervical cancer and vaginal bleeding and keeps on dropping her hematocrit as we give her blood. So I decide waiting isn’t helping her so I decide to proceed. We give her two bags of blood then start the surgery. As the foley is inserted it drains blood. I re-look at her carnet (medical booklet) and it definitely says vaginal bleeding with mobile cervical cancer. So I open her abdomen and find a small uterus. And something hard in her omentum. I take the hard part out of the omentum and don’t find any evidence of metastasis on liver or peritoneum. I clamp, cut, tie down the sides of the uterus and each tie really stresses my fingers again. These also stress my finger ligaments as it takes a lot of force to tie these tight so the vessels won’t bleed afterwards. Finally I come across below the uterus, cervix across the vagina. I look at the cervix on the specimen and it looks normal. Hmmm, well sure doesn’t look like cervical cancer to me. Back to ? Bladder cancer. I can’t feel anything abnormal in the bladder. But Ive decided even if I see a bladder cancer again I will likely not do any surgeries for it. It is many hours of surgery and I don’t want to do anymore ileoconduits and don’t think it really prolonged their lives in the past. So I close. Even tonight as I type I can feel my index finger is tired.
I do the other prostate guy in the same way as above.
Then the last one of the day is a 20 something woman with huge swelling of her face she says has gone on 3 years. And worse these past 4 days. So does she have a cancer that now has become necrotic?? So many unknowns here! I did an ultrasound yesterday and think there may be an abscess underneath. With the most being right where the facial nerve lays in front of her ear. Her eye is puffy and I think it must be pus.
While Im waiting for her to be ready I see many consults. One sticks out in my mind. It is a guy who has a cancer on his nose. Dr. Denae biopsied and sent to Ndjamena and apparently it is a squamous cell carcinoma. He smells awful! His septum has been eaten away. I think that if I do an aggressive resection I may be able to get it all but he will have a horrendous looking face afterwards. Maybe if he survives, someone could do a plastic reconstruction afterwards. So I offer a very disfiguring surgery to them and the want it! I have a difficult time explaining what he will look like afterwards, but they want to proceed. I take about 45 minutes to explain. They go to pay for the surgery. God help me to get it all out and for it to be worthwhile for him to be disfigured like this!
The girl is ready and so she is given propofol and ketamine. I cut into the side of her face in a way that I think won’t hit the facial nerve. I stuck a needle in and so I know there is pus down there. I go deeper and deeper and eventually hit pus. It flows out. It was a significant pocket. As I flush it out, the nurse thinks the fluid is going into her mouth. Wow, these neck infections and dental abscesses are awful! Ive seen so many this time. I pack the hole and she goes out when she’s awake.
Another dental abscess is draining on another patient’s mandible and we pull out a piece of dead bone out of her upper neck. These people desperately need dental care!
I think there are only a handful of dentists in the whole country and likely most are in Ndjamena.
I will do the nasal cancer guy tomorrow. God help me!! I need your knowledge! I’m so inadequate to deal with so many things here. HELP ME!