9 Bere 2024
I did a prostatectomy yesterday and as I usually do, I put the foley catheter on traction, with the foley bag always being half full and laying over the end of the bed. So i was called in at 8:30 pm because the guy was crying in pain. I know that none of the prostatectomy guys like traction, it always hurts. And of course they are getting the only medications we have for pain here which are Ibuprofen and Tylenol. So I go in to see him. They have it off traction and are trying to flush the catheter. I take over and get red blood with clots out of the foley. Im really frustrated as it’s not on traction and so it’s bleeding more. I know if it bleeds to much and isn’t flushed out- then the clots collect in the bladder and then Id have to reoperate and clean out the bladder again. I decide that the next nurse is coming on shift in about 15 minutes. Im so tired, so rather than hanging around I go home and lay on the concrete floor. I wake up 3 hours later in a pool of sweat. I remember that I needed to see the patient so I go back in. He’s writhing around in pain. His foley is plugged! I unplug it and am glad I went in to see him. I discuss with this nurse what to do if it plugs and she seems much more attentive than the last nurse. So I head back and shower and get in bed dripping wet, It’s still 98 deg in the house when I go to bed. But I fall right to sleep.
Im awakened at 5 AM with the maternity nurse who says there is a new patient who has a dead baby and has hard contractions and isn’t progressing. Audrey went in to see that patient and was back soon saying that the patient had a dead baby and had a ruptured uterus. So I called in Phillipe and David and about an hour or more later we were beginning the surgery. As I cut into the abdomen with a phanynsteal incision, as soon as I enter the peritoneum- lots of blood. I feel around and find the dead baby floating around in the abdomen with the placenta. Again the uterus is torn up the side, just like the one yesterday. I find the deep spot and put ring clamps all along. Then I start closing. I get the uterus closed and then oversew a few bleeding spots. Audrey is assisting me and we close up the abdomen. She goes off to check on another patient that has had her first 4 children die during child birth. I see some consults and she comes back and tells me she wants to do another C-section on this one so she will have a live baby. They are just ready to put in the spinal of my next patient- so we get that one off the table and get the next C-section going.
We know the baby is not in distress so we take our time getting into the uterus. We see a little meconium (baby poop) on the kids face- so there was fetal distress! He has a nucal cord (umbilical cord around his neck) so I reduce that and pull him out. He cries immediately- yay! A live baby! Audrey and I close back up. It’s about noon when I start my first case that was planned that day.
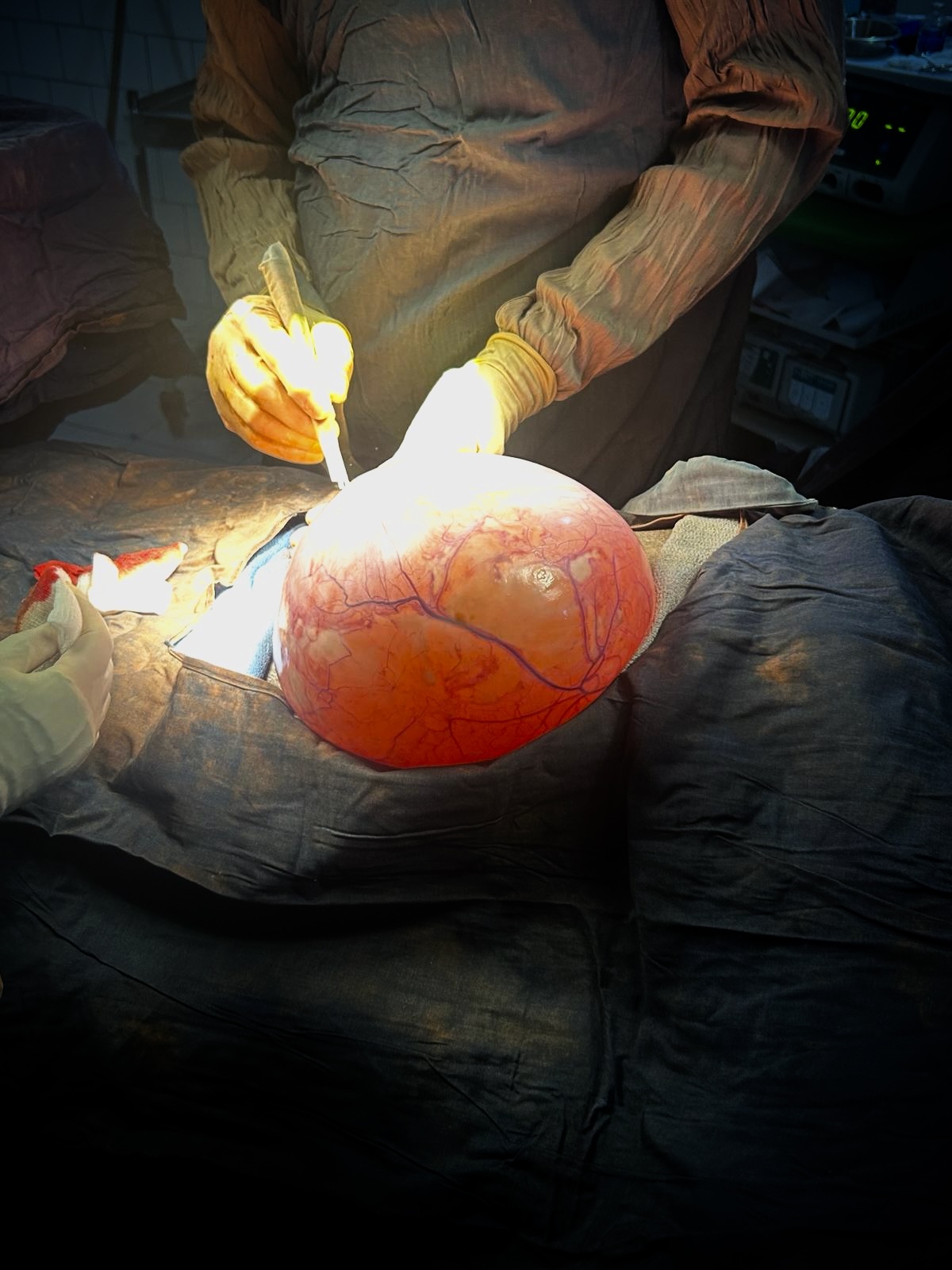
this woman has had a large abdomen for quite some time. Ultrasound says it’s a large cyst. Must be ovarian! I open her thin protuberant abdomen. Immediately there is a huge cyst in my view. I open nearly from the pubis to the xyphoid. Then im able to pull it up. It’s about the size of a basketball. I release omentum from it and then find it’s attached in two places. I tie off these areas and get to lift it out of the abdomen. Im guessing about 15lbs. Her abdomen went from looking pregnant to looking scaphoid.
I go out to do some more consults and I find a guy sent over by the ER because he has a leg infection. It appears he has drop foot and hasn’t walked for a while. he says his legs have been infected 2 months and he hasn’t walked for a month because of pain. I try to figure out where his pain started, what part of his leg. It takes a lot of questioning as the nursing student translating for me I think is asking something different than what I said. After about 4 minutes of talking I think it started at his knee then later he had pus coming out in different areas of his leg. I ask to have him taken into the OR. I see another couple of the consults as they get him ready with fluid and a spinal anesthetic. They call me once the spinal has been placed. The anesthetist walks out of the room shortly there after and is going about 10 minutes. Where did he go? He went out.. is the answer. Out where? We don’t know. Rather than getting upset like is my instinct when this happens- i keep my cool and just watch the BP when it cycles and listen to the SAT monitor. The guy remains stable as he had been given enough preload of fluids. I start with the knee joint. I try to pike a needle attached to a syringe in to get a sample of the knee fluid to see if it is obvious pus. His leg is so swollen I cant seem to get it in the joint, or at least I cant pull anything into the syringe when i think Im in the joint. But I decide it is suspicious enough that I open the side of the joint beside the patella anyway. I do get some pus. So I wash it out with dakins and put in a piece of sterile glove as a drain. The remainder of the leg is swollen. So I aim for the draining holes. I probe each one with a forcep and then open along the direction of the largest part that avoids important structures like names nerves, names arteries, or named veins. Of course there is bleeding from smaller vessels but packing the abscess sites helps stop that. After I follow about 7 draining sites and open them, I cant feel or tell of any other place that needs to be opened. So Ive packed them all then I wrap with elastic bandages. It’s about 6 PM and I’ve gotten through the consults and surgeries so I head home to eat whatever Longue has made and am content to have a seat and some rest.