Shanksteps Bere April #12 with pictures
I go in for the last day at Bere Hospital before I leave. Went to morning worship then back to my room to prepare stuff while they have another meeting. When I go back in I do rounds with Abouna, a nurse who does quite a number of surgeries as he’s been trained. He’s quite intelligent. I do rounds with him so that he knows what I plan for each of my patients and can tell the next surgeon when he comes next week.
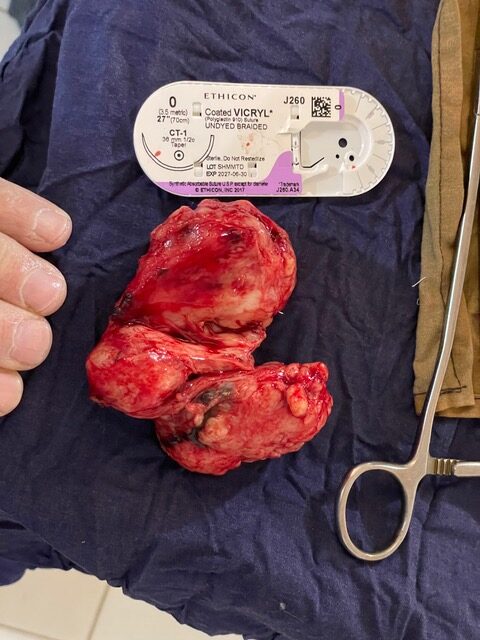
The first patient is ready, he’s an old tall Arab guy with a large prostate on ultrasound and can’t pee. I start to cut his abdomen and though the nurse said he was ready he feels it! So I wait till he gets some ketamine before I continue. I make a phanynsteal incision, cutting down through the skin and fascia, split muscles along the midline and then spread above the bladder sweeping the peritoneum and intestines up and away from the bladder. I open the bladder and suck out all the liquid we’ve put in the bladder to distend it. I feel inside and feel a huge prostate. Hmmm, is this cancerous? I don’t feel nodules, but it is large. Slowly I break the anterior prostate and gradually shell it out with different fingers. As each one gets tired, I use a different finger. Usually my right index and middle fingers. I have to make my incision in the bladder a little larger as it won’t come out of my original size incision. After removing it, I sew up the back wall down low where most of the bleeding occurs. Blood is constantly welling up and it’s hard to see. Eventually with the stitching it slows down. I put a new foley in and inflate the balloon. I check to find that both ureters are still putting out urine and I hadn’t caught either one in my stitching. They are working well, so I close the bladder in two layers like usual. I leave a piece of sterile glove as a drain and close up the rest of the layers, irrigating at each layer. We take him out to the “recovery room” and bring the family in to show them how to take care of the bladder irrigation. It’s sad that I feel more confidence in the family doing well with the irrigation than the nurses. But the families here are used to caring for their patient and they’re invested. Once they understand what I want them to do they usually do it. It just takes repeated translations to tell them. And I do it differently than Dr. Denae, leaving the foley on tension, so it’s a learning curve for the nurses too. Once I think the family understands, I see some consults about a leg mass, neck mass, infertility, a hernia, Then go into the next surgery that’s ready.
The next was an old lady with a black dead foot. Yesterday when I saw it, it was dry gangrene, dead and shriveled black without an odor. Today the whole pre-op area smells like dead with pus! Wet gangrene. She is taken back and a spinal anesthetic done. Her below knee amputation goes well. There isn’t as much blood flow as normal so I wonder if she will heal this amputation site. I do it with a nursing student as Abouna had to go to the government office because he’s involved in some sort of land dispute. They call him and say come now, so he leaves work and goes and deals with it. A few hours later he’s back at work. The student helping me is helpful, but I have to direct him quite a bit on what to do.
I see some more consults, and then there is a older woman with a hernia in her central abdomen about the size of a foot ball. Initially when I saw her I wasn’t sure wether this represented a hernia or a mass, but I suspected hernia. After her spinal we are able to reduce it, hernia! I cut down into the large fat layer and gradually around the hernia sac. I open and resect the large sac. I then close the fascia with a large suture. I suspect she may have a large seroma (fluid collection) in the fatty layer, so I leave a piece of sterile glove as a drain.
One of the consults I see next is an old guy who can’t pee. He says he had a foley catheter in that didn’t work but when they pulled it he had a lot of blood in his penis. Once again I be the foley was placed and the balloon blown up below the prostate and not in the bladder. Then suprapubic foley was placed. He hasn’t been able to urinate with his penis since. The foley in the lower abdomen fell out a week ago. He went to the hospital in Kouseri (Cameroon) and they wanted 200,000- 300,000 CFA ($400-500) for the surgery to fix him. He decided to come to us about 12 hours away. But it took him about a week to find money and get here. He says that he can’t pee and small amounts of urine come out his abdomen. I do an ultrasound with my Butterfly and see a very full bladder up to his naval. He pays at the pharmacy for a foley and bag and I take him into the operating room as I know this will be difficult as the tract has closed up. I anesthetize his skin and cut back open the skin. I know Im going to do this blind along a tract that has closed, but I hope I can re-open it and get a foley in the same place. So I probe the tract with a sterile heavy blunt probe that usually used for vaginal stuff. Im gradually able to shove it down the tract into the bladder. I feel a pop then pull it back out. No urine. I know I was in deep enough it was easy after the pop. And I know I have a huge target of urine to hit. So I put the heavy probe down a foley catheter and push it down. It’s tight but I think I get it in. The probe is difficult to pull out. After getting it out- only a small amount of urine in the foley. I use a force to cram more foley in the hole. Urine comes welling up in the foley. I very grateful. I blow up the balloon, which doesn’t cause any pain, so the balloon is in the right place. He drains about 2 liters of urine and feels much better.
I look at the registry of surgeries since Ive been here. 35 surgeries in 2.5 weeks. That’s a good number. I’m looking forward to being home with my wife and in cooler weather.
Pic of large prostate and a prostate patient.