What an irregular day- it began normal and ended with me putting a chest tube in and taking a bullet out.
The first surgery was a boy about 5 with a bladder stone. Operating on the smaller ones isn’t fun for me as everything is small. A small incision, a small bladder, a small opening- making it difficult to see and operate. But I pulled a stone out of his bladder about 3/4in in size.
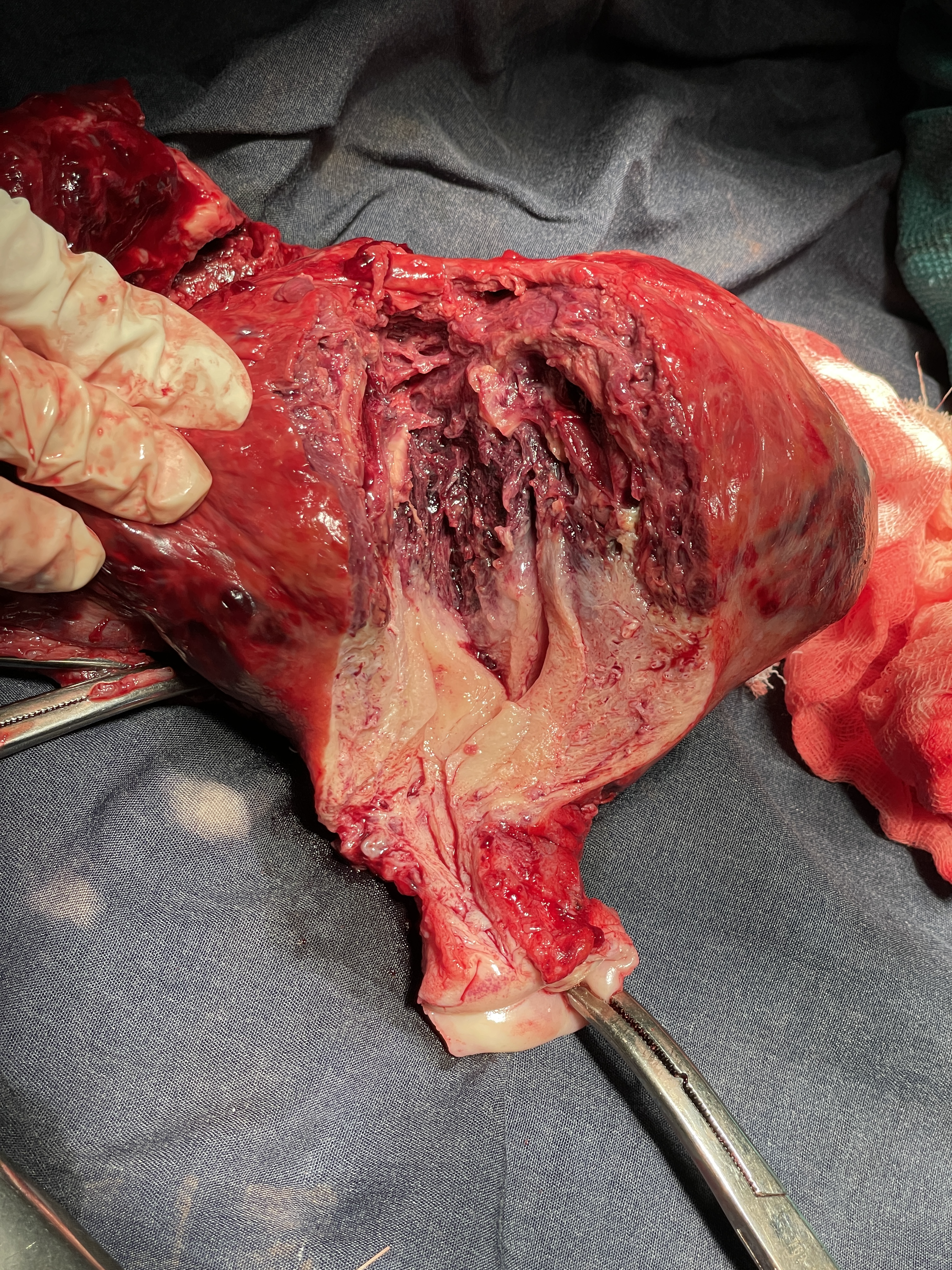
Next was a 65 year old woman with a uterine cancer as was seen on ultrasound. I also did an ultrasound and just saw a lot of irregular tissue in the pelvis. It seemed mobile so I decided to try and take it out. Upon entering the abdomen, I find old blood and large old clots. The bottom of the uterus seemed normal, but the top was very large. I gradually worked around it and freed it up from the omentum and small intestine that were stuck to it. Now it looks somewhat like the top blew out of the uterus. We work down either side and eventually get to the end of the uterus and cervix. I suture up the tissues and look for bleeding. There is a little so I tie that too. My resident, Anna, says there are studies now that say the fallopian tube can get ovarian cancer. So we take the remaining fallopian tube, leaving the ovary. I seem to remember that the ovary helps with osteopenia (weak bones) in post menopausal women.
Audrey asks me to see a guy on the adult ward that has severe abdominal pain and has typhoid, and peritoneal signs (perforated intestine?). I go to see him and he’s sitting up eating bouie (This is like a rice/flour/peanut porridge) Hmm, If he’s really sick he shouldn’t want to eat. He tells me his pain has been intense like this for two weeks. He hasn’t been vomiting but once yesterday. He has had some diarrhea, and also had some today. He says he keeps down small amounts of food over these past two weeks. His abdomen is quite tender with percussion tenderness, guarding and no rebound. I’ve seen this before with someone here who just had very irritated intestine from their typhoid. At the operation on that person they had red irritated bowel but no perforation. I do a bedside ultrasound and see no fluid in the abdomen. I order a upright abdominal X-ray and am told by one nurse we cant do those and only flat X-rays, and by another we can. I head back to the operating room where they are preparing my next patient.
I see a man in the pre-op area that has blood flowing out his foley catheter. I ask the nurse who put in the foley if they blew up the balloon before or after getting urine/blood. He says the guy has had frank hematuria for 4 days and worse the last two days. There was straight blood coming out before he inflated the balloon. I do a rectal exam and feel a very large prostate which is very soft. Prostate cancer is my first suspicion and prostatitis my second. I don’t know if prostatitis can cause frank hematuria. I have the nurse put in a three way foley and start bladder irrigation. Either way the type of prostatectomy I do, won’t help with a cancer as it leaves the capsule. So I’ll treat him for prostatitis and hope that it stops. I’ve had very poor internet while here, so I can’t look up things like I’d like to.
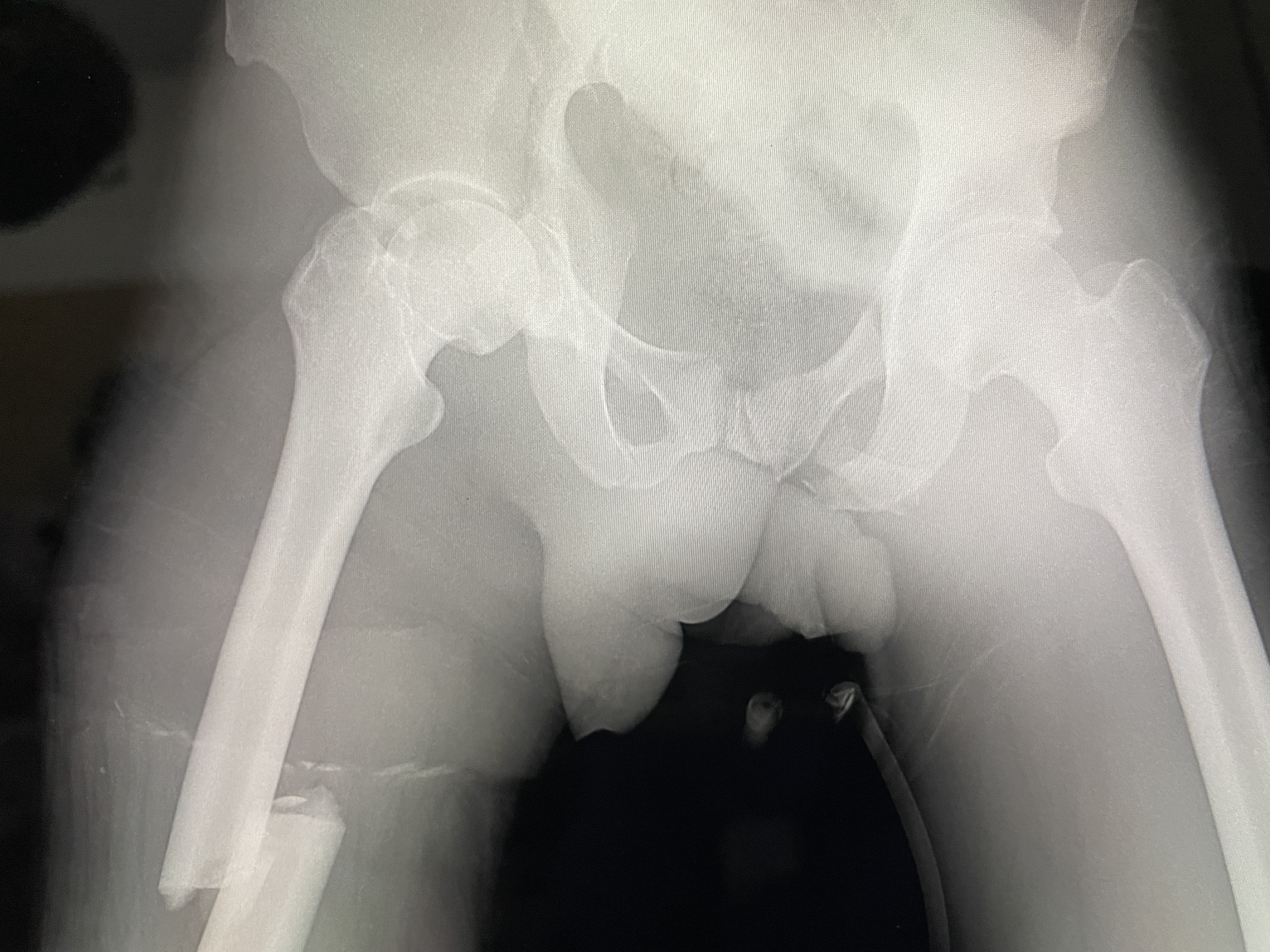
I walk back in to the OR and my next patient who has a pelvic fracture and a broken femur is sitting up because the anesthetist wants to put a spinal in. I’m shocked that he sat up at the anesthetist’s insistence with a broken pelvis. Since he’s already sitting up I tell Phillippe to go ahead with the spinal. This guy was making mud bricks at the edge of a large termite mound. They can get about 7-10 feet tall. As he dug out dirt from it, it fell on him, breaking his femur and pelvis. He came in with the traditional wood splinting. I asked the nurses what the traditional healer would charge to do that and they guessed $40 equivalent. We took off the splint and prepped his lower leg and I put a steinmen pin in the tibia for traction. I’ll send a picture with either this email or the next with him in his bed. It was quite a work of ingenuity, that involved a number of people.
Then there was a guy who had been about 10 hours north about a week ago. There was conflict in the area and he was shot. Apparently he had a chest tube that was taken out and he made his way down here to be treated. The nurse thought to get away from the area of conflict. He has a whited out lung and a bullet in his back that’s palpable. My student went away to the house of the guard to have some goat. So I put in a chest tube in the OR and took out the bullet. I got about 400ml of dark fluid (old blood) out. I incised the area of his back with the bullet and pulled out what looked like a 223. He was breathing better at the end of the procedure. He walked to the surgical ward with his pleuravac canister in hand.
God, please give us wisdom to help these many different diseases and unknowns!