6 bere 2024
It’s my least favorite thing here in Bere, neck abscesses from dental cavity infections. I am sitting in the worship area which is a metal awning outside the ER. Someone is giving a worship thought to the hospital workers in French and its translated into Nangere, the local language. Im distracted by chickens walking by and pecking at something on the ground next to me. There is a muslim man sitting in the front row waiting for the ER to open and just stayed there when worship started. Another younger muslim guy walked up and starts talking to him, someone asks him to be quiet as we are having a meeting. Then one of the nurses that asked me to help him with his schooling last week, walks up to me and says his uncle isn’t doing well and would i come see him. I had admitted the uncle the day before. He had swelling of his chin and neck and I did an ultrasound and didn’t see anything to be drained. It had be the rotten tooth cause. He couldn’t open his mouth for me to see anything in it (trismus). So I treated him with IV antibiotics. I go over to where he is and his family is carrying him from under the tree to his bed. He is sitting rocking back and forth and looking weaker and weaker. They get a sat monitor and his sat is 47. He is dying… I tell them to carry him to the OR NOW. they grab him and I run for the OR. I get the stuff and as soon as he’s on the table I try to intubate him. I don’t expect to be able to open his mouth at all and also think of an emergency trach. But I try, and it opens some. My mac intubation blade is to small. I find another and try again. I intubate him and we start CPR. The nursing student stays in the room and the other family members leave. I pray for God to save him as I do chest compressions once the anesthetist is there to bag him. I switch off with Audrey and a couple of OR guys. We do chest compressions and bag him for more than 30minutes. His pupils are fixed and dilated. We stop. He is still dead..
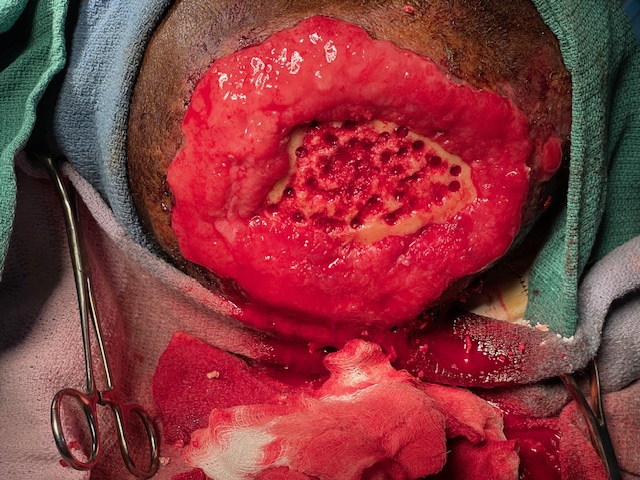
Another of my least favorite is a similar issue of a woman who was admitted over the weekend. I found her on rounds Sunday morning. She had an ace bandage around her neck that was wet with pus and her whole upper chest area was red and was like a big fluid pocket- pus! So I told her to not eat or drink anything and she needed to go to the OR. I wanted to sedate her but when in the OR i realized she couldn’t open her mouth but about a quarter of an inch. So I cant sedate her and she will have to be done with local anesthetic. This never works well, but is what is necessary. The OR staff doesn’t want her in the OR because she smells awful, like dead flesh. (Think decaying animal). So we do it on a bed in the consultation room. She is sitting leaning against another woman. I put betadine on, I know is useless, and then inject lidocaine in a few areas. This is painful and she pushes me away. She says she is going to die. I think to myself that she probably will. I incise the different areas that I injected and cups of pus flow out. There is a dead patch of skin on her neck and I cut that off with scissors. I realize that when she coughs a well of pus flows up from behind her sternum. I see dark black tissue bubble up too. I grab it with a forcep and pull up a huge piece of dead tissue from behind the sternum. I grab the Dakins bottle (dilute bleach) and drown the area with it. More pus flows up and out from behind the sternum. The guy standing by helping hold her and the woman holding her, both nearly pass out. The stench is awful. im glad we are not in the confined room of the OR. After there is pus everywhere and I cant smell anything but dead smell, im done. I’ve pack everything I can and I go to wash off all my exposed skin I can. I don’t think i got it on my skin, but I feel very dirty…
So i hate that the people here have no available dental care or way of getting to it. And even when they have rotten teeth they often want to keep them because they’re the only teeth they will ever have. We, in the first world countries, are very blessed to have access to care many other people in the world have no access to at all.
God help me to demonstrate Your love to these suffering people!