Bere 2024 #3
Warning graphic!!
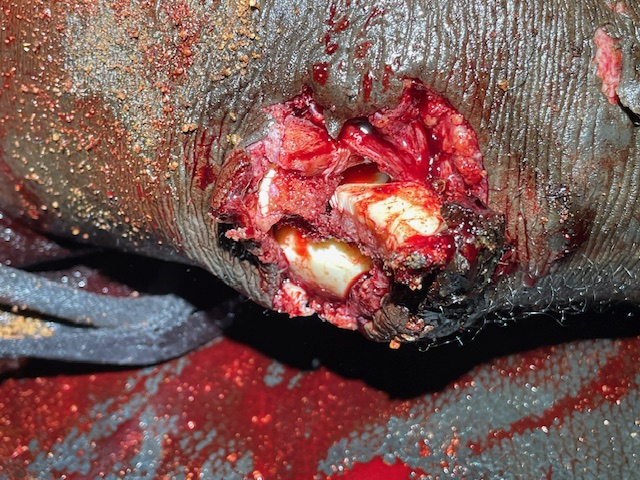
Ohhh, Noooo! I walk into the preop/recovery room and Dr. Steven is looking at a guy laying on his stomach. It appears like the mans anus exploded! what happpenneddd? He was riding a bike yesterday when he fell of and the pedal went into his anus. It looks aweful with loose tissue hanging all over. he has a urine catheter that has blood in it. I see Dr. Stevens examination and its clear there are more than one hole and its kind of difficult to see what is actually the anus into the rectum. So we decide to do the hystorectomy case that is already in the OR ready then we will do this guy.
The hystorectomy is the third case of the day. We did a mastecomy first on a lady with inflammatory breast cancer which is considered pallatative- not for cure but to give her a better life for a little while. I was able to remove the breast and get some enlarged lymph nodes out of her axilla (arm pit). It was a bit snug getting her skin back together, but was able to do it. And i left a piece of glove at the bottom to come out as a drain.
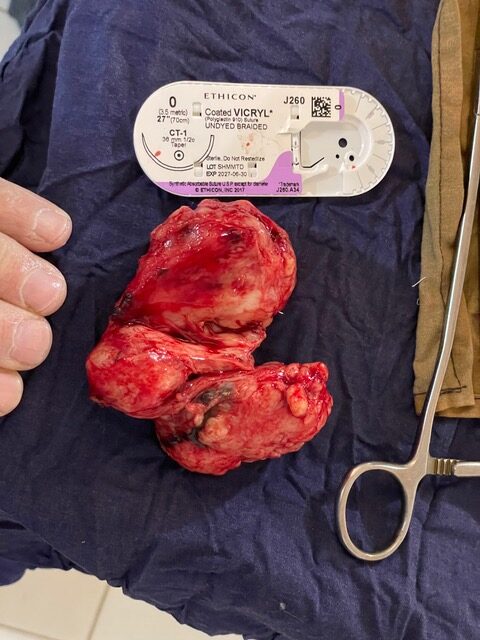
The next lady had a mass in the pelvis that a previous doctor had thought was uterine in nature. So we took her to the operating room to attempt to remove it. As I palpated her abdomen it seemed to be about 10 by 12 inches in size and didn’t want to move around when i pushed on it. So i imagined it was fixed to surrounding structures. After she has her spinal anesthetic placed by the anesthetist she is laid down and her abdomen is prepped. Next I get scrubbed and put on the cloth gown and my sterile gloves. I put the cloth drapes on the patient and we begin. After we pray for our patient I make a vertical abdominal incision. I go through the skin, then a tiny layer of fat, then fascia, then into the peritoneum (inner layer of abdomen). Next i see intestines and after sweeping them to the side with my fingers, I feel the mass. It appears cystic and it is stuck all along the right side. i can feel around the back side and it seems there is space behind near the rectum. Slowly I make an incision along the right side and slowly make it down to where the iliac artery and vein are. I find there seems to be two main cysts. Im able to slowly go inferior to the cyst and the later and find the two main cysts off in my hands. Below that is the uterus that looks fine and the left ovary is normal. So I close up the fascia, and skin and she goes out to the recovery room.
Next is the guy with the bike pedal to the rear end. He gets a spinal anesthetic after enough IV fluids were given. Then he’s put up in stirupps flexing at the hip so we have a good view of the anus. It really does look like an M80 went off inside. I swipe poop out of the way and spray down the hole with Dakins (dilute bleach) solution. As I look around the anus, I realize there’s a hole anterior to the anus and then realize that the hole is between the prostate and the rectum. The prostate normally is directly next to the rectum. How did he get a hole between two small structures the don’t come apart easily. As I evaluate the rectum it appears intact. I think a diverting ostomy would be best, but after discussion with the doc that’s always here, decide to not do that yet. An ostomy is hard to have here as there are minimal ostomy supplies available so no real seal on the abdomen. I have patients at home that will give me supplies, but it always seems there are more important things to take in my ?6 pieces of luggage. I decide to leave a large drain deep in the hole and suture it out to the skin. Then I excise the dead tissue and suture skin back to the anus- or whats left of it. I sincerely doubt he will have any continence, but then again, there did seem to be a little anal tone left. I had warned the patient before the surgery that I thought he may be incontinent after this accident, forever.
i go out to the preop/postop room and start seeing the different surgical and medical consults that are there. A young kid with a vascular mass on his inner thigh, a kid with enlarged cervical nodes, an old woman with abdominal pain going on 3 years, a 30yo man with an abdominal mass that fluctuates in size and i think i see a mass on ultrasound, an old guy with eye itchiness and a cornea that is completely whited out…. After about 10-15 pateints i head towards home and make it about 20 feet.
The nurse from maternity sees me walk by and says “doc I was just going to look for you” Well it was said in French…. So there is a woman who has just arrive with her 4th pregnancy at about 8 months and shes having vaginal bleeding. The babies heart rate is normal, but blood and clots continue to come out. She’s not in labor and is at one centimeter cervix dilation. They just are drawing a hemoglobin level and getting an IV going. I do a bedside ultrasound with my Butterfly (small ultrasound that i attach to my iphone). I find the placenta appears intact and not covering the cervix and babies heart rate is good. I decide to go get some advise from my wife and another nurse here. I find them painting a house in preparation for a doctor that is moving here soon. After their advise I go get some supper of rice and beans and then go back to see what the hemoglobin and results are. She continues to have bleeding. So i decide to do a C-section. I try to call the two guys back to the OR. I cant get either one. So the nurse goes to use the “hospital phone”. It has no cell credit so they cant make calls either…. I ask the maternity nurse to do something or send someone. Normally I’d be quite mad by now, but I made an internal pact to push gently when encountering problems here this time and let people make poor choices if they make them. So i sit for about 45 minutes before the scrub tech shows up. Then he tells me he also does anesthesia now if I can find someone else to assist me. So I go find Audrey and ask her to assist. She is willing and eventually we start. I make a low pfannenstiel incision (bikini) and go down to the muscles. I divide them along the middle and open to the uterus. I make a low across incision on the uterus and get immediately quite a bit of blood. OHhh, placenta abruption (the placenta separating from the uterus and it bleeds in between). I find the bulging sac of amniotic fluid and open it. Gush, I feel the blood and amniotic fluid run over the front of me and I feel the wetness through my gown from my belly button to about mid thigh. I don’t like that feeling! That’s the side effects of cloth gowns- not impervious at all! I pull out the babies head and suck out the nose and mouth. Then pull the rest of the kid out. She starts to cry as we cut the umbilical cord. Yay!! A live baby! So many come so late that we doctors usually see the worse cases and baby deaths. The normal deliveries are done by the oncall nurse. I pass off the baby to the nurse near by. Audrey and I then close the uterus and then the abdomen. Mom and baby are doing well. I head home to slow down and shower and get to bed late. It was a long but good day


.