
Shanksteps Bere April #11
I started an audio book in the evenings called Cross and the Switchblade- about ministering to NY gang kids. Im finding it hard to put down to write you all 🙂 I want God to use me like he did David Wilkerson. Not for kids in NY but however He sees fit.
Today God is using me to help individuals here with their diseases that I can help with surgically. I make rounds while I wait for the OR crew to get the patients ready. I start at 8:30 after they’ve had their morning meetings. At 7AM I went to the Hosptial worship. It is singing a song in Nangere and then a worship thought that someone has prepared which is translated from French into Nangere. Or vis versa if the speaker is Nangere. During rounds I see the guy with the open below knee amputation that I amuptated for wet gangrene of his diabetic foot. Now he’s granulated and free of infection so it’s time to close it. I send him to the OR for preparation. I check on the guy who had pancreatitis and had a lot of pus out his abdomen yesterday. I see intestine at the wound site- oh no a dehiscence and eviceration. I tape a dressing on him tightly and send him to the OR so he can be operated on today as well. He just ate bouii, so he’ll have to wait till later. The teen with the open neck wound and a feeding gastrostomy tube is doing well so far just very weak from lying around. The kid with the leg burn that I did the release on is doing well but not walking yet because of pain. I encourage him to walk. The old guy with head trauma still hasn’t woken up yet, so we continue IV fluids. The family wants to give him water orally, I strongly discourage this as he will aspirate and then die, which he may anyway! I see the kid that I opened the femur on for osteomyelitis drainage and do his dressing. He tolerated it really well but screams at one point. The people here are so tough!! His mom cradles his head as I change his dressing. There are so many painful dressings here, and we can’t take all of them back to the OR for changing as there is to much to do and I don’t want to give sedation I their hospital bed for fear they won’t be watched and could die. They are used to doing dressings on the ward, and I do it in spite of the pain I’m causing him. Of course him living with osteo that is draining at different points on his leg is also painful. So he has dealt with pain a long time.
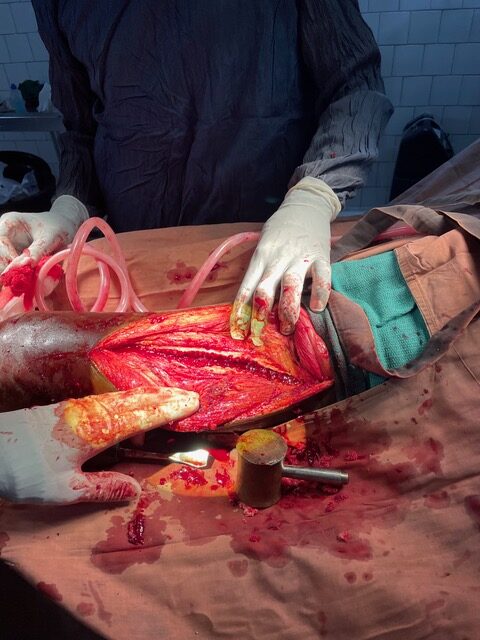
The first surgery is that of the below knee amputation. He is given a spinal by David and then his leg is prepped and draped. Then I cut off excess muscle and bring up the flap. It has shortened some with time so it’s a little tight to bring up to cover the opening. With a bit of effort and suturing, I bring the edges together leaving a drain going along the base inside.
Next is a woman with osteomyelitis of her mandible with draining sinuses. I explore this and nibble away at rotten bone. Its is somewhat helpful I think but it’s really when there is a sequestrum (dead bone that has separated) that I feel like Ive really done something useful for them. She also needs her teeth pulled that are the rotten source, I leave this to the nurse who does that. Though the OR isn’t a bad place to do this! I pack and put tape on the dressing.
Next is the older guy with dehiscence and pancreatitis. I had pulled his pancreas drains a few days ago as they weren’t functional any more. After his spinal, we prep his belly and opening with betadine. Then as I look in is see my suture intact all along with a rim of fascia just ripped off one side. Did he do a sit-up and just rip it off, or did the pancreatic juice make the fascia weak, or was it the subcutaneous abscess that did it? Likely a combination of all of this I guess. Either way I debrede off the edges and take out the previous suture. I re-close his abdomen with retention sutures and a fascial closure and leave the skin open for packing between them. I hope this one doesn’t fall apart. If it does he may need to be dressed open and I guess that will be the next surgeons problem as I leave soon.
Then there is a patient that hasn’t progressed as needed in her labor for a child. So she is brought to the OR by Dr. Staci for a C-section. As she does the C-section I see outpatients that have waited all day since morning. In between seeing the patients with STD’s, infertility, neck mass, goiter, kid who can’t pee (stone), large inguinal hernia…
I go and check on how the C-section is going. I see the local doc giving a mask to the baby who is blue and not breathing. He is shoving the mask onto the face of the baby tilting the head forward and trying to mask him. I ask that the oxygen be brought, and I take control of bagging the baby. I tilt the head back to open he airway and mask effectively. Pulse ox that I have put on shows oxygen saturation of 72 (normal above 92). A nasal cannula is put under the mask and I bag for for a while till the saturation is normal and the kid appears to be breathing on his own without masking. I explain to the students how to position the head for masking, and hope the doctor is listening. I leave to go back to the consultations. I see a older woman with a huge abdominal mass sticking out how her fat abdomen. It’s likely a huge hernia that won’t reduce. Another 27 year old woman has uterine prolapse after a delivery of a dead baby. Another has vague abdominal pain that “starts in my legs, goes up my abdomen to my chest then back to my central abdomen” I treat him for typhoid and worms. I often find descriptions of symptoms amusing and also difficult to figure out what to do. But with limited meds, I choose what’s available and likely to help.
God help the people I’ve seen today to heal and gain their health back. Help them to know how much You love them! Give me Your words to speak to them!




{kind=link}
{kind=link}