Bere 5/2025 #10
A MIRACLE! Thank you God!!!!
I attend the morning worship and concentrate on listening to the one translating into French. He reads a worship thought from a book called the Desire of Ages, a book about Jesus. At least that’s I think what he’s reading from. All the book covers here look different than ours so I’m not sure. As I listen to the worship thought, daily life is going on past me on the other side of the fence that is around the hospital. Horse and cow drawn single axle carts go by. A small pack of dogs bicker with each other. A young man appears to be harassing a woman who then picks up a small switch and goes after the young man. Everyone is laughing except the woman who must at least be insulted. A moto taxi pulls up with a couple people on it, bringing them to the hospital. I find it hard to concentrate on the message as my brain is all over the place.
After worship there isn’t any meeting so I go to the OR and tell them Im ready to work. I do this to help them get going, otherwise they linger and do whatever else they do in the morning. Like talk to a patient that is a friend and gab a while. I also go by the surgical ward and tell them Im ready to round. This gets both locations going. But I just stand around waiting in the surgical ward. So they get going. The dressing cart is prepared faster and Emma changes from his street cloths into his scrubs and we start. I see all the patients Ive already told you about. The guy that was gored by a cow horn is better but is complaining of pain on his side where he was gored. Some pus is coming out the drain I left. But as I look with a flashlight at his dark skin, I realize he has some dead looking skin on his flank. It looks like he was burned. I asked the family and they decline knowing anything about it. They’ve been very attentive to this man. There are at least two people fanning him day and night. It’s nice to see them so engaged. I’m not sure what to make of it. I wish I had a CT scan…… and so many other things to diagnose him further. He’s still eating some boui (porridge) and pooped yesterday. Great signs. I’ll keep an eye on that spot. I leave most of the dressing changes for the nurse to do. The next one is a woman who is a sister to Emma. She had a thyroidectomy and we are certain the recurrent laryngeal nerve was cut which was repaired and would make a person hoarse. She seemed hoarse the first day and now her is clear! It’s a miracle!!!! I’m excited to share this with the one who did the operation. It has been many stress filled days of knowing this woman will be hoarse for months or permanently. BUT SHE IS HEALED!!! We have been praying for that. Thank you God!!!! We pray for so many people to be healed of physical or spiritual things and I don’t understand why it happens like this some times and other times it doesn’t. But I’m so grateful to see healing when I do. Later that day I share it with the surgeon and we just sit in the moment of relief and thanks to God!
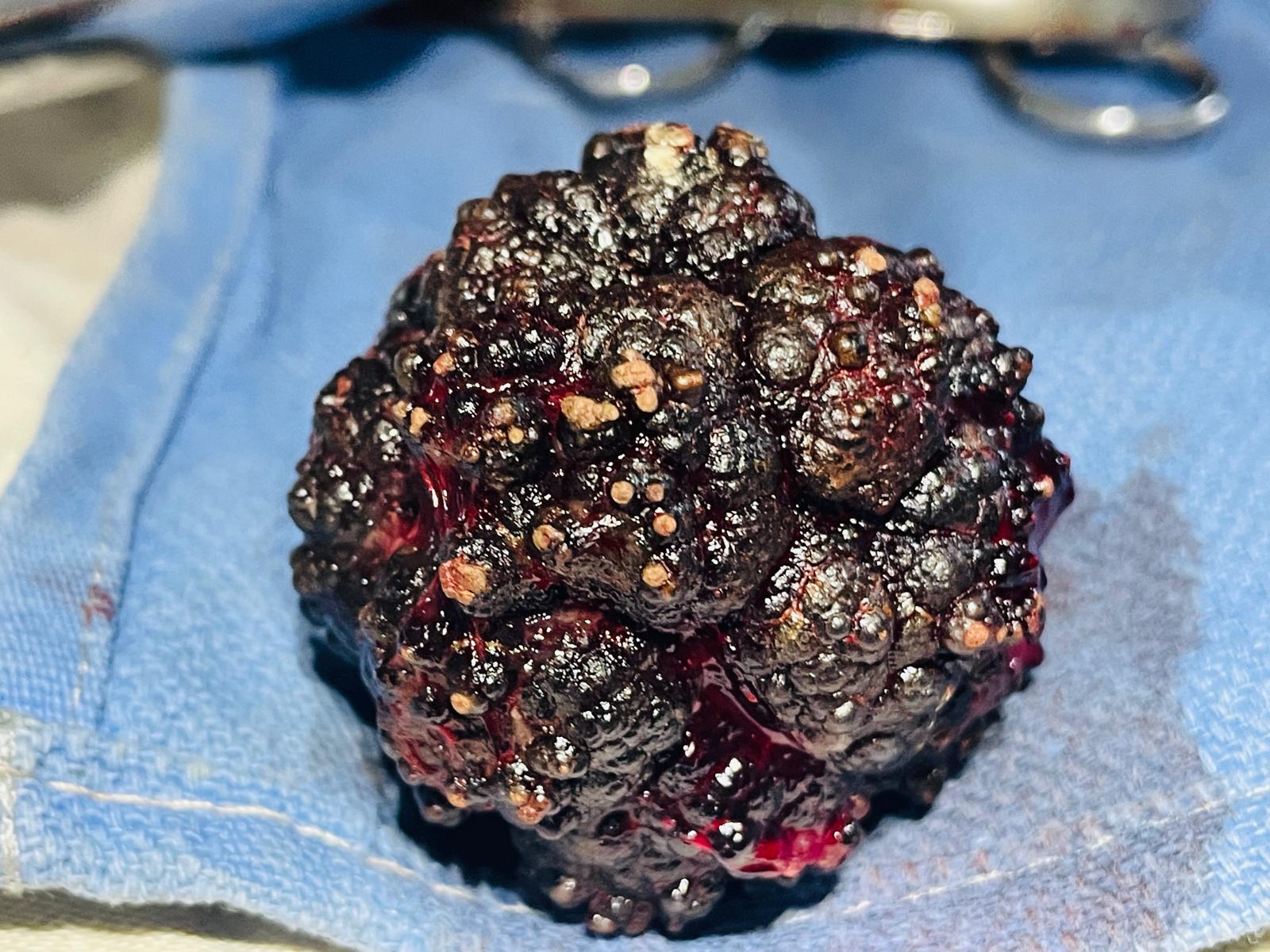
Back to the OR and they aren’t ready yet. Phillipe is concerned that we are starting a long difficult abdominal surgery and since the generators have been cutting in and out the last many days- is it safe to do this surgery. He mentions that there is a generator specifically for the OR that hasn’t been started in about a year. Could we make sure that one is functional first. I think that’s a good idea. So I ask Dr. Andrew how to arrange that, he makes a call then goes off to find out. As always, missionaries, have so many different tasks to manage, and are pulled in so many ways. It would be so much less stressful, if we were able to only stick to what we know- medicine…. So we prepare another patient in the second OR. This one is a TURP (transurethral resection of the prostate). We figure if the power goes out we can stop that surgery in the middle if we have to. He is also known to have a large stone in his bladder too. So the first patient waits all day and we never do get the go ahead from a generator standpoint. So he is postponed till the next day. The prostate is slowly shaved off using that same method I described in my last email. Only this time each movement I make is bumping against a bladder stone. If feels large, but then again, everything is magnified in this cystoscopic image. It takes us a few hours to complete the resection of enough prostate so he should pee well. We search many times for the ureters and never find them. Thats a crucial part of the surgery. So we are continuously bothered by that. We need to see them and protect them. But the stone has created so much inflammation we can’t identify them. So we stay more in the middle where we know they aren’t. After we decide we’ve done enough for the exposure we have. Then we transition to the surgery on the abdomen to remove the stone. After going through all the layers of the abdomen and bladder, I try to grab and pull out the stone. It is large and I have to enlarge my bladder incision twice before I can pull it out. It is about 2.5inches wide and black with lumps all over it. Each bladder stone is different and this is unique in it’s color and shape. Wow, that must hurt being in there, and have been in there a long time.
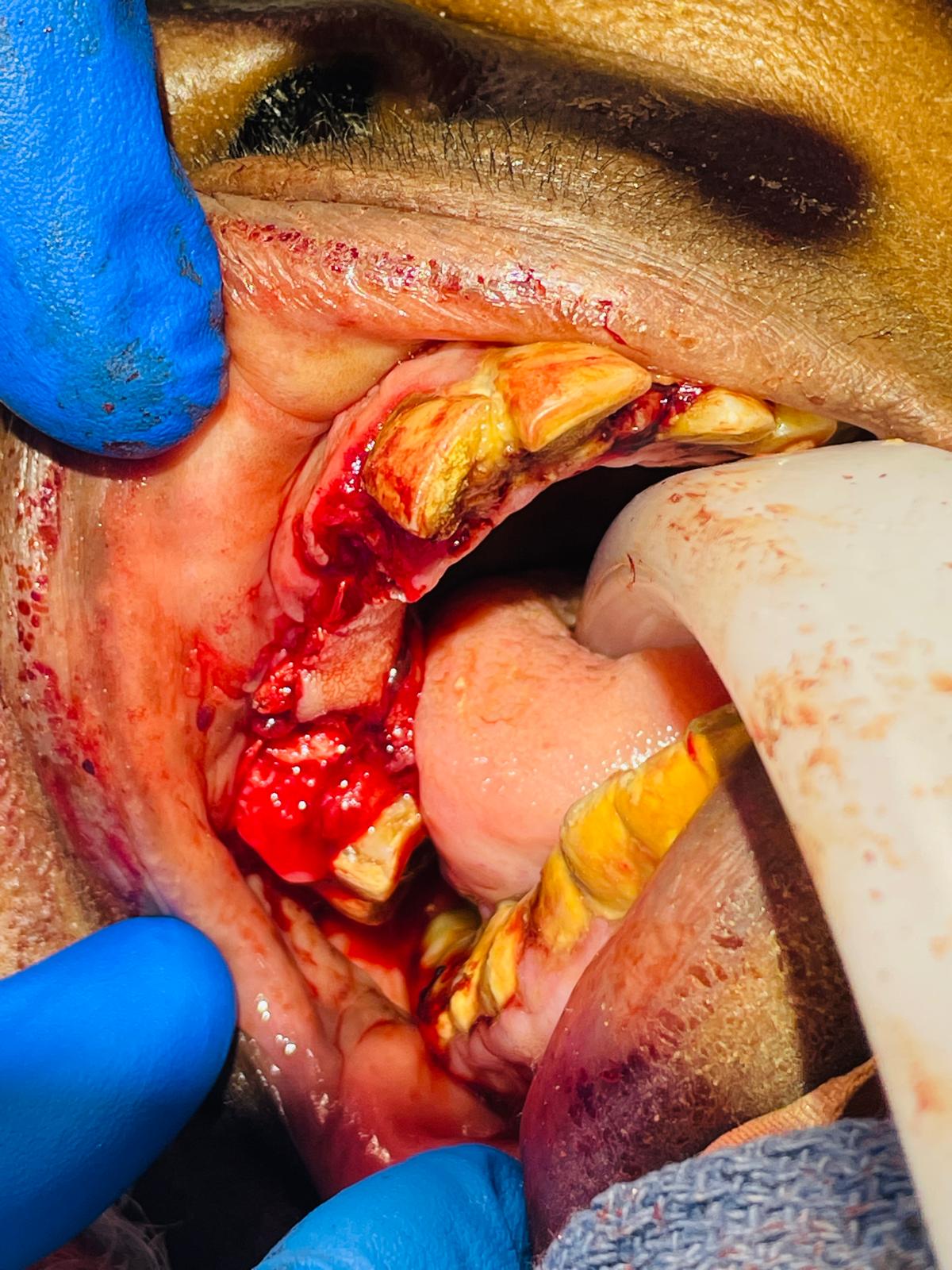
The next patient needs a foot debridement. No one in the room really understands her language. So what I hear is she was normal 4 days ago then she an infection started. I take off the cloth she has wrapped around her foot and the whole top of her foot is dead. Dead skin and pus everywhere. (I’ll attach pictures). Zach and I use scissors to cut away all the dead stuff till we get to bleeding, live tissue. It smells awful!. We chip away at the dead stuff till it looks much cleaner but I’d be surprised if she doesn’t need a foot amputation. I bathe the food in Dakins solution and then put wet dressing. Ill check on her in the AM to make sure her infection isn’t getting worse or one of the rapidly progressing necrotizing infections. Later in the night I’m in seeing another patient, and I see her leg is already less swollen than it was at the time of surgery…improvement. I’m grateful! Thank you God for the improvements I see in our patients. The others are so hard to see and it’s great to see the good ones. God give me strength for the bad outcomes too. Amen